
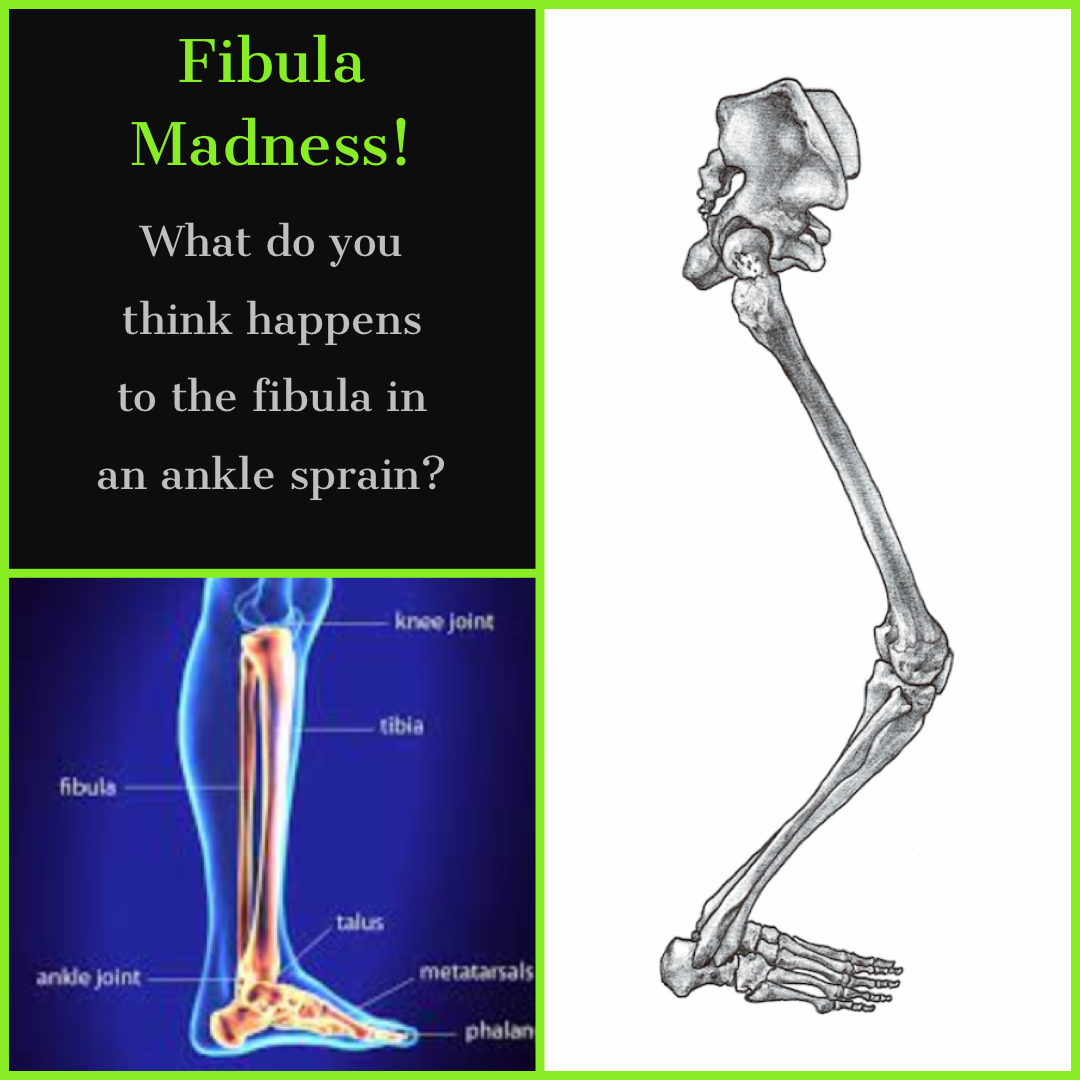
Fibula Madness


How do I put a big red X through this image? 👆🏼
Ankle sprains are notoriously challenging for people and in my experienced opinion NEVER treated well if at all (unless you consider RICE, ankle circles and standing on a wobble board a treatment 🤷🏻♂️) I apparently do not.
Ankle sprains are one of the more damaging, long lasting and far reaching injuries that we can do to ourselves and most people shrug them off and get back to sport as soon as they can walk/ run again. Because we can. Yes. Because the body is amazing. Yes. And yet in it’s amazing-ness the body adjusts itself to accommodate your now poorly treated ankle sprain.
What can we do better? Well, job number one is to directly assess the ankle. It is made up of four bones: tibia, fibula, talus and calcaneus. Classically the ankle roll, tips the calcaneus aggressively towards the outside (inversion), dragging the talus with it and pushing the distal fibula away from the tibia and dragging it downwards away from the knee. Consider all of the muscles, tendons and ligaments that have been yanked around as those bones push and lean into them. YOWZA! 😣
So when you are wobbling about on your wobble board and doing ankle circles… it might be worth considering that the bones in your ankle may no longer be in an optimal position and to become aware that the wobble board is NOT going to put those bones back where they belong. So you could be strengthening your ankle in a less than optimal structural position…. 🤔
Your amazing body will quickly have to respond and reorganise itself to accommodate this change in your structure. Do you think you would have confidence standing and bearing all of your weight on a leg that has experienced such a violent moment? Do you think that the ankle just slots itself back into place? And when your whole body adjusts to accommodate the injury, do you think that just because it’s now ‘feeling better’, it will revert back to its most optimal position?
This blog is about two people I saw in quick succession: a guy who’s fibula post ankle eversion sprain was causing havoc in his system.. and a lady who’s inversion sprain tipped the balance in the later foot border of her foot.
Let’s call the guy Sid the surfer. Well, he is a surfer. Sid has been struggling with knee pain, hip pain, groin and upper lateral, low back pain and neck discomfort for a number of years. He has seen everyone and manages it with massage, rest when he really needs to and some good old Aussie spirit (basically F it, I’m going surfing).
Check out our courses if you want to learn about the AiM Method and Flow Motion Model.
It was one of those assessments where you hear the phrase “sprained my ankle and was out for months”, and I think to myself. That’s it…. rule it in or out and then move on.
So I assess the ankle, as described above that requires a check of the resting position of the tibia, fibula, talus and calcaneus.
I consider the fibula an extension of the lateral border of the foot. The lateral border of the foot includes the 4th and 5th metatarsal, the cuboid and the calcaneus. An ankle sprain is so detrimental to this part of the foot as well as the ankle that I always consider these bones as well.
Allow me to digress a moment, to share that a lady last week had recently rolled her ankle and could simply not weight bear on her foot at all. But not in the way that she couldn’t stand on her foot, she couldn’t stand on the outside of her foot (lateral border). So I checked her lateral border and noticed instantly that she doesn’t have a palpable Styloid Process on the 5th metatarsal. What? 🤯
She has one on the other foot so why not this one? Every one has one right? Thankfully I have seen this before on several occasions. An inversion sprain, classic roll of the ankle, can invert the lateral border sufficiently enough to invert the fifth metatarsal so that the Styloid process actually points downward instead of to the side. So what she couldn’t bear weight on was actually the sticky out part of the fifth metatarsal that shouldn’t be there in the first place. A quick block of the cuboid and eversion back to neutral of the 5th met and all of her weight bearing issues went away…. this was in less than 10 minutes. After two weeks of “keeping it up” and “resting”. I hope you can see that no amount of rest, makes this problem go away. And if the therapist isn’t looking for it. They simply won’t find it. You could see it in the x-ray (but only if you compare left with right.
⏺️⏺️⏺️⏺️⏺️⏺️
Back to Sid the surfer. A similar issue is to be had. The sprain of the ankle in this instance was an eversion sprain, which oftentimes leads to a fracture of the distal fibula head, but in this instance it forced the fibula upwards, forwards and outwards at the ankle and upwards, backwards and inwards at the knee. Again on palpation, the proximal fibula head very clearly wasn’t where it is supposed to be. Instead I could feel it located on the posterior lateral corner of the leg maybe 5mm to 10mm back from where it should be 😳
It takes something remarkable for me to want to sit down and write about it 😆, this was remarkable.
Symptoms of knee pain, hip pain, low back pain, upper back, neck and shoulder pain are all present SINCE this injury occurred.
When Sid’s back hurts, the back is treated, when he goes for a session with shoulder pain, he’s given a band to work the rotator cuff. Knee pain ➡️ stretch and strengthen the quads and hamstrings 🥱
I promise you if the fibula is out of place, the idea of doing any of that is simply futile.
The fibula is often overlooked. After all it’s just this non-weight bearing bone on the outside of the leg, right? This line of thinking will simply not do. Much like dismissing the talus as the ‘dumb’ bone… just because it has no muscle attachments. But when your primary thought pattern is “joints act and muscles react” – you quickly realise that the talus is boss. All bone and no tissue. I often joke that the tibia is the real dumb bone. That big lump just piggy back’s around in the back of the talus, with the oh so dextrous and refined fibula floats alongside it…. but not in Sid’s case! The malpositioning of his fibula comprises its movement, freedom and elegance, hugely compromising the rearfoot, lower limb and knee… limitations in the movements of which will compromise the hip, pelvis, low back and up through the rest of the body to the neck and shoulder too. Reminder to treat the cause of the problem rather than just throw the same old exercise at something.
When the foot pronates in gait there is a specific shape adopted by the leg and this includes the fibula (Check this out on my lower limb biomechanics online programme). As this pronating leg occurs, the fibula slides vertically up and forwards at the proximal knee end. Given that Sid’s fibula was pushed up and back into the corner. That’s one huge block on his ability to pronate that leg. This is marked by his inability to evert and internally rotate his rearfoot, it is also apparent in his ability to move his pelvis and spine in ways that match the flow of working with a pronating leg rather than against it.
As each assessment adds up to not being able to pronate that leg, we start to have a pretty good idea of what needs to be done (if it wasn’t already obvious that is!)…
❌ Lack of hip hike on the same side
❌ Lack of rotation away from the pronating leg
❌ Lack of anterior tilt on that side
❌ Lack of lateral flexion and rotation towards the pronating leg
These all point to the fact that he cannot pronate his leg, so the quest is to find out why? But with the fibula in that position it should become crystal clear that that alone is blocking up the whole system. And since all discomforts began to arise AFTER the ankle injury, we have a cut and dry focus for the session.
These assessments are all covered in our online programmes




So what do you do?
✅ Knowing the movement requirements of a bone and it’s surrounding joints is key to making that decision.
✅ Knowing the integration between the bones that lay in sequence is also going to help.
When you bring that fibula head forward (even manually), begin to consider what should the knee be doing, what would the rearfoot be doing, what about the forefoot? Bring it all together into an integrated movement pattern. If I try to slide the fibula forwards on an externally rotated femur for example, I simply block and hinder my own progress…. As we slowly re-educate the fibula to glide again in its fabulous and dextrous way, we can reconnect it to surrounding structures and ultimately bring it back into uproght and closed chain movement to teach the whole leg, pelvis and spine to come along for the ride. Consider just how much tissue can get involved now that these new movement sequences are put in place. Consider that all bones and joints have the freedom to come out of their limitation and explore new territory, loading and unloading muscle tissue, ligaments and tendons – all previous held captive under the spell of an ankle eversion sprain.
The response in Sid was immediate, his relief palpable and feedback wonderful. He called me a magician… but there are no secrets to this work, just follow the bones, understand the bones and learn how they sequence together through the gait cycle which I documented for you many years ago in my Flow Motion Model
Come and learn with us, check out what’s available both online and in live classrooms.
Continue Your Flow Motion Model Journey
👣 The FMM is discussed in my book What The Foot? which is also available to read online here.
👣 Download the Free 7-steps to take ownership of your body. Access the free ebook here
👣 Get started with our self-assessment programmes for Every body.
👣 Check out our live courses page to find out how to access a live course with an AiM teacher
Leave A Comment